
You’re Looking for 8 Hours of Sleep. But Your Timing Has Been Totally Off.
Science may have been answering the wrong question the whole time. How the domains of Adaptive Resilience synchronize into a rhythmic life.

You’ve been told to sleep eight hours. You might be tracking that number on your wrist right now. The advice is not wrong, exactly — but it is measuring the wrong thing.
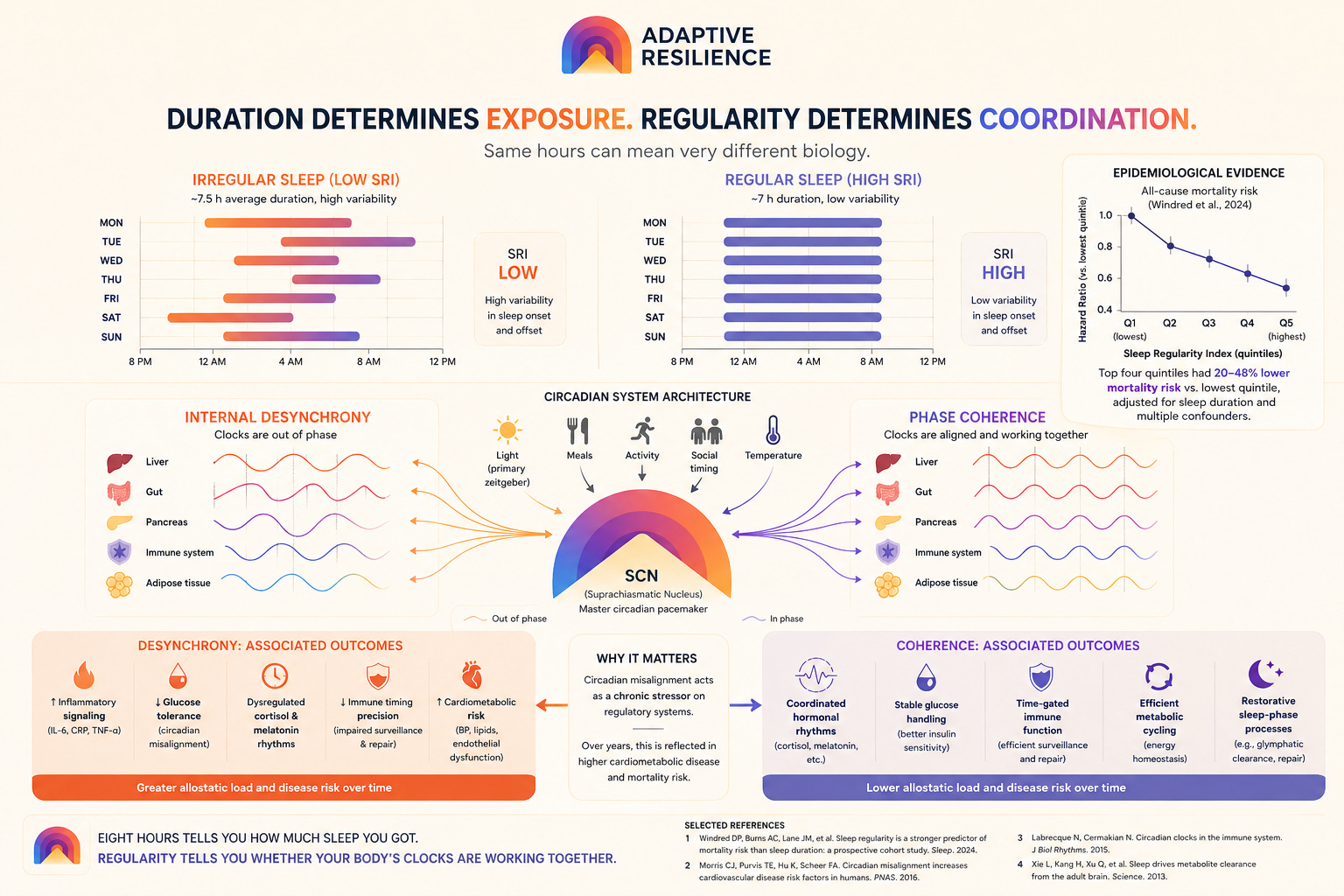
In 2024, researchers tracking 60,977 people in the UK Biobank for over seven years found that sleep regularity — how consistent your sleep timing is from one day to the next — predicts mortality far more strongly than sleep duration. The people in the highest regularity quartile had up to 48% lower risk of all-cause mortality than those in the lowest quartile, after adjusting for duration and the usual confounders. [1] That is not a marginal effect. That is a large, durable signal hiding inside a variable that most health advice (or device) does not even measure.
The variable everyone has been optimizing for two decades is downstream of a simpler one that almost no one tracks.
Sit with that for a moment. Then think about what it implies for what sleep actually is.
What regularity is, and what it isn’t
The Sleep Regularity Index is not the same as going to bed at 10:00 PM on the dot. It is a statistical measure of how similar your sleep-wake pattern is from one day to the next — how much of your sleep timing is structured rhythm versus how much is noise. [2]
High regularity does not mean absolutely no variation. It means your biology has a pattern it returns to. A consistent anchor. The difference between someone who lands in bed between 10:30 and 11:00 pm most nights and someone whose schedule drifts by two or three hours depending on whether it’s a work night, a weekend, or a travel week is not just a difference in discipline. It is a difference in what their circadian biology is doing under the hood.
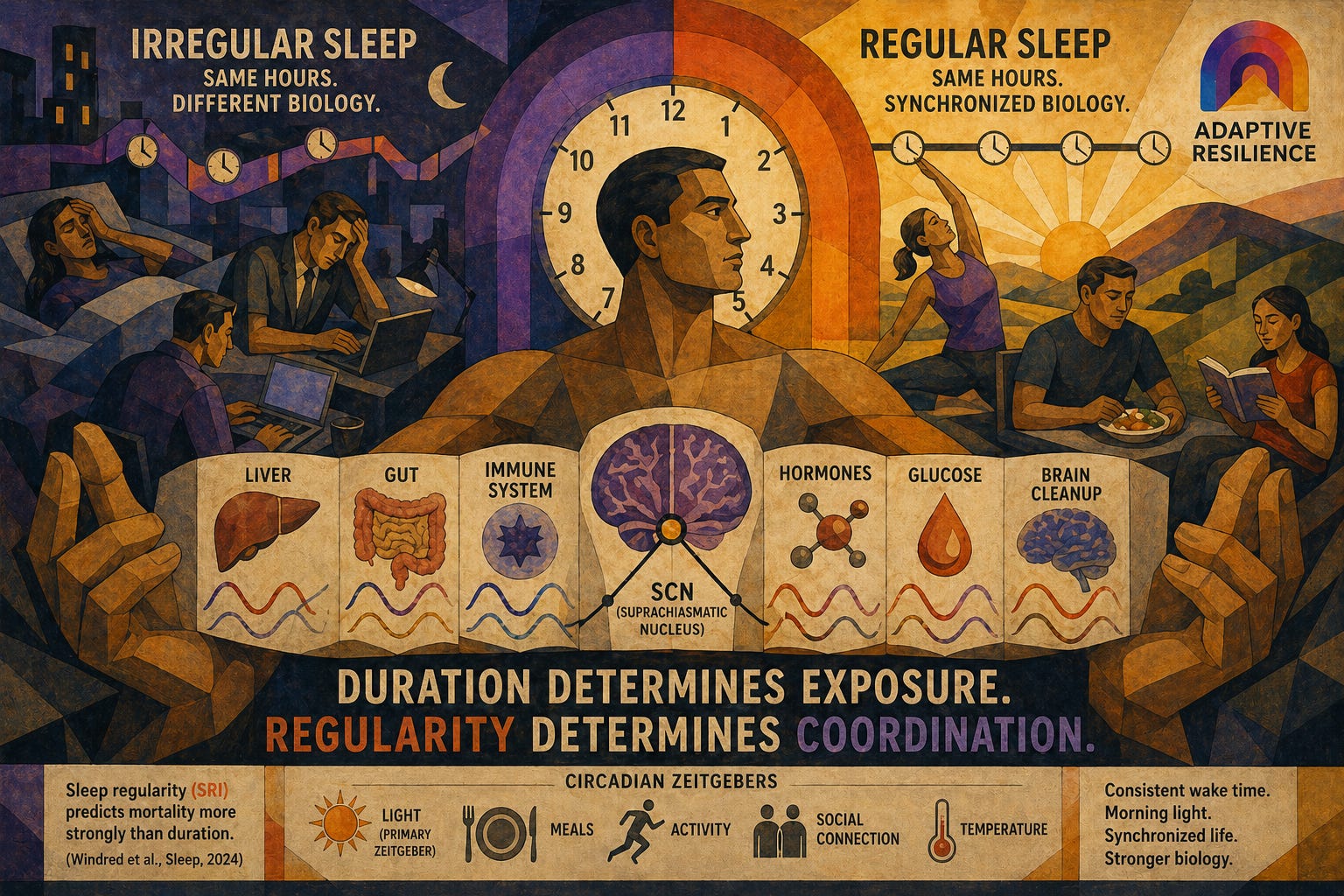
Your circadian system is not one clock. It is a hierarchy of clocks — the suprachiasmatic nucleus in the hypothalamus acting as the master pacemaker, and peripheral clocks in your liver, gut, kidneys, immune tissue, and almost every organ following its lead. These clocks synchronize to each other and to the environment through a set of signals called zeitgebers — light exposure, meal timing, physical activity, social contact, temperature. Sleep timing is one of the most powerful of those signals. [3]
When sleep timing is irregular, the master pacemaker and the peripheral clocks fall out of phase with each other. The liver thinks it is one time. The immune system thinks it is another. The gut operates on a third schedule. Chronobiologists call this internal desynchrony, and the phrase deserves more weight than it usually gets — it is describing a body in which the trillions of cells doing trillions of timed things are no longer agreeing on what time it is. Two people who each logged seven and a half hours last night are not biologically equivalent if one of them shifted three hours from their usual.
What mortality really measures
The Windred et al. 2024 paper (UK Biobank, n=60,977, seven-year follow-up) is the largest prospective cohort study to put regularity and duration head-to-head as competing predictors of mortality. The result — regularity wins — survived adjustment for age, sex, education, employment, body mass index, smoking, alcohol use, physical activity, and existing comorbidities.
What makes this finding worth pausing on is what mortality is a proxy for. All-cause mortality, and cardiovascular mortality in particular, is the slow, accumulating signature of metabolic dysfunction, inflammatory burden, and immune senescence over years and decades. It is a long-tail variable. The fact that sleep regularity tracks it across seven years is telling you that irregular sleep is not just an inconvenience the body shrugs off. It is a chronic stressor on regulatory systems that, given enough time, depletes their capacity.
The mechanistic literature points the same direction. Internal desynchrony elevates inflammatory markers. It scrambles the timing of cortisol and melatonin secretion. It impairs glucose tolerance — not because of what you ate, but because your peripheral metabolic clocks are out of sync with insulin signaling. [4] It interferes with the glymphatic system’s overnight clearance of metabolic waste from the brain, which runs on a sleep-phase-dependent schedule. [5] It degrades the immune system’s surveillance and repair functions, which are also time-gated. [6]
None of this shows up in a sleep duration metric. Eight hours of irregular sleep does not buy you the same biology as eight hours of regular sleep. The hours are nominally the same. The system underneath is not.
The mistake in the “eight-hours” frame
Here is what the eight-hours story implicitly assumes: sleep is fundamentally a quantity. A tank you fill. Get enough of it and you are covered.
The regularity data points to a different architecture. Sleep is not like a fuel tank. It is a timing signal your biology depends on, layered on top of a duration that determines how long the biological processes run. The processes themselves are gated by circadian phase. You cannot get the full benefit of sleep at the wrong phase, and “wrong phase” is not just a function of when you went to bed tonight. It is a function of how much your system trusts that tonight’s timing means something — how strong the pattern is that it has to anchor to.
Your circadian system is, among other things, a forecaster. It pre-positions metabolic and hormonal resources based on anticipated timing — gearing up insulin sensitivity for an expected meal window, ramping cortisol for an expected wake, releasing melatonin in advance of an expected sleep onset. A regular sleeper’s biology has a stable forecast and trusts it. An irregular sleeper’s biology is constantly recalibrating, never fully confident in the next prediction, never fully optimized for the upcoming window. The cumulative regulatory load that this recalibration produces, summed over years, is what the mortality data is capturing.
This is the part of the picture that has not made it into the mainstream conversation. Sleep is not just rest. It is a coordinating signal for almost everything else the body does in time.
Why this is foundational for every other domain
Adaptive Resilience is built around eight domains — sleep, movement, nutrition, mental load, social connection, physiological stress, recovery, and growth. The framing of this series is that they are not eight independent levers. They are parts of a synchronized whole, and sleep regularity is where that synchronization becomes most visible.
Irregular sleep degrades almost every other domain. Cognitive sharpness, emotional regulation, appetite signaling, motivation for movement, and the capacity for warm social engagement all show measurable circadian sensitivity. [7] They are not just impaired by total sleep loss — they are impaired by circadian misalignment even at adequate total duration. An athlete training consistently, eating well, and managing stress but sleeping irregularly is leaving adaptation on the table, because the biological integration of those inputs runs through the same circadian systems that irregular sleep continuously perturbs.
This is why sleep regularity is not one of eight equally weighted inputs. It is the rhythm that conditions the return on every other input. When the rhythm is intact, the rest of the work composes. When the rhythm is broken, the rest of the work delivers only a fraction of what it should.
The substrate underneath all of this is neuroimmune — the systems that govern inflammation, hormonal signaling, metabolic timing, and the cellular repair processes that express during sleep. The previous post in this thread, on ibogaine and developmental inputs, was about that same substrate seen from a very different angle: a window briefly opening to let it reorganize. Sleep regularity is the daily, unspectacular version of conditioning the same substrate. Maintenance, not intervention. The two are not in competition. They are different time-scales of the same architecture.
What this looks like in practice
The most useful thing about the regularity finding is that it suggests a different intervention than the duration finding does.
If you cannot directly control how long you sleep — and most of us can’t, at least not consistently, and not without practice, because insomnia, stress, kids, partners, and life often interrupt our own health — you can usually control sleep timing more than you think. The primary lever the regularity literature points to is a consistent wake anchor. Same wake time, weekdays and weekends, even after a short night. The wake anchor stabilizes the master pacemaker. The master pacemaker re-synchronizes the peripheral clocks. The peripheral clocks resume their coordinated work. A consistent morning light exposure in the first hour after waking — bright daylight, ideally outside, even briefly — locks the signal in.
This is not glamorous advice. There is no supplement. There is no hardware. The intervention is a simple phase anchor and a willingness and intention to benefit from it.
What the data also suggests is something most sleep advice will not tell you out loud: a 6.5-hour night at a consistent time is not obviously worse, on the long-run metrics that mortality is a proxy for, than a 7.5-hour night at a variable time. It may be better. The hour you would have spent sleeping in is, from your circadian system’s perspective, an hour of confusion that ripples through the rest of the week.
What I am doing with this
A few years ago, my sleep tracker said I was getting just nine minutes of restful sleep a night. Nine minutes! I was dealing with a months-long chronic illness, and I found sleep regularity impossible to maintain. After nearly a year of emphasis on fixing my sleep, I now fall asleep almost as soon as my head hits the pillow. Feeling well-rested every day always feels fantastic.
I track a Sleep Regularity Index score derived from nightly wearable data, using the same methodological approach as Windred and colleagues — how consistent is sleep onset and offset from one night to the next, across a rolling window. A high SRI score means the system has a stable anchor. A low SRI score means it is in chronic recalibration mode.
The reason regularity is a first-class metric in my practice, alongside duration and the usual sleep stage breakdowns, is that the literature now supports treating it as the primary signal rather than a secondary one. The eight-hours story made sense given what was known fifteen years ago. The story now is more interesting and more actionable. Quantity buys you exposure to the biology of sleep. Regularity buys you the integrated function that biology produces.
Adaptive Resilience as a framework is built on the bet that the long-run metrics — flourishing, durable capacity, healthy aging — are mostly downstream of regulatory architecture rather than individual heroics or willpower. Sleep regularity is one of the cleanest examples of that claim. A boring intervention with a large mortality signal, sitting underneath a domain everyone is already paying attention to, that almost no health system measures.
The strange thing about the eight hours
If you take one thing from this post, take this: the question worth asking at night is not how long you slept. It is what time you slept, what time you woke, and how close that pattern is to the pattern your biology is expecting.
The mortality data says that question matters more than the duration question. The mechanistic data tells you why. The intervention is free (maybe a sun lamp for higher latitudes and winter months). The cost of not intervening is measured in the same currency as everything other harmful thing slowly accumulating in your physiology.
Most of the work of Adaptive Resilience is like this. It is not that the conventional advice is wrong. It is that the conventional advice is sitting on top of a deeper layer that almost no one names — and the deeper layer is where the leverage is. The reason this newsletter exists is to map that deeper layer, one domain at a time. If that is the kind of map you want, subscribing puts the next entry in your inbox when it lands.
A note on sources and framing
The mortality finding [1] is established peer-reviewed evidence — a prospective observational cohort, not a randomized controlled trial. It establishes a strong epidemiological association with prospective design and a large sample, but not causal mechanism on its own. The mechanistic account of internal desynchrony is supported by separate experimental literature in animals and humans, cited below.
The frontier claim in this post is not the underlying study. It is the architectural interpretation that sleep regularity is the foundation under the other domains of Adaptive Resilience, rather than one input among many. That framing is a working hypothesis of the Adaptive Resilience model. It is consistent with the mechanistic evidence and parsimonious with the mortality data, but it is the layer where I am furthest ahead of consensus, and the reader should hold it accordingly.
Sources
Windred DP, Burns AC, Lane JM, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep. 2024;47(1):zsad253. doi:10.1093/sleep/zsad253
Mortality risk reduction by SRI quartile; regularity vs. duration head-to-head; UK Biobank n=60,977, 7-year follow-upPhillips AJK, Clerx WM, O’Brien CS, et al. Irregular sleep/wake patterns are associated with poorer academic performance and delayed circadian and sleep/wake timing. Sci Rep. 2017;7(1):3216. doi:10.1038/s41598-017-03171-4
Original derivation of the Sleep Regularity Index methodologyPanda S. Circadian Code. Rodale Books; 2019.
Circadian hierarchy, peripheral clock synchrony, and zeitgeber overviewMorris CJ, Purvis TE, Hu K, Scheer FA. Circadian misalignment increases cardiovascular disease risk factors in humans. Proc Natl Acad Sci USA. 2016;113(10):E1402–E1411. doi:10.1073/pnas.1516953113
Internal desynchrony, cortisol/melatonin disruption, and metabolic/cardiovascular markers in controlled human experimentsXie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. *Science.* 2013;342(6156):373–377. doi:10.1126/science.1241224
Glymphatic clearance and sleep-phase dependenceLabrecque N, Cermakian N. Circadian clocks in the immune system. *J Biol Rhythms.* 2015;30(4):277–290. doi:10.1177/0748730415577723
Immune system circadian gating; time-gated surveillance and repair functionsSpiegel K, Tasali E, Penev P, Van Cauter E. Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004;141(11):846–850. doi:10.7326/0003-4819-141-11-200412070-00008
Sleep and appetite hormone signaling; leptin/ghrelin disruption with sleep loss